Rapid Reference
- Zugang+BE: BGA, min. 2x2 [BK|Blutkulturen], Profil “Sepsis”
- Bedarfsgerecht VEL bis 30 ml/kg je nach Volumenstatus
- NA Push-Dose / Perfusor peripher frühzeitig bei persistierender Hypoperfusion oder Hypervolämie, Ziel-MAP >60-65 mmHg, ggf. +Adrenalin/+Vasopressin
- Urin: U-Status+Kultur, ggf. DK-Anlage (Diurese?)
- Fokussuche mit Anamnese, gründlicher Untersuchung, POCUS, Radiologie, ggf. weitere Materialgewinnung (Sputum/TBS, LP, Aszitespunktion etc.)
- Kalkulierte Breitband-ABx nach vermutetem Fokus (Ziel: <3h, <1h bei Schock)
- Reevaluation: Lactat, MAP, Urin-Output, VTI? Übersehene DD? Fokussanierung?
DD Sepsis Mimics
“Sepsis kills! … but it doesn’t kill Patients who don’t have Sepsis.” –Cliff Reid
- Anaphylaxie (Abgrenzung u.U. schwierig, ggf. empirisch +Adrenalin i.m.)
- Kardiogener Schock (TTE)
- Infektiös
- Infektion ohne Organdysfunktion
- PJP (Immunsupp., atypische Pneumonie, LDH↑↑)
- Invasive Aspergillose, Invasive Candidose
- Endokrin
- GI
- Sonstige: z.B. HLH i.d.R. erst intensivmedizinisch relevant
Anamnese
- S: OPQRST+? Schmerzen? Fieber/Schüttelfrost? Husten/Auswurf? Dysurie? Wunden?
- A: insb. ABx?
- M: Immunsupp.? Interaktionen Hausmedikation-ABx?
- P: (Relative) Immunsupp. (z.B. Tx, Diabetes, Alkohol)? Rezidivierende Infekte? Vorerkrankungen (z.B. Divertikulose)? OPs/Eingriffe/“Spritzen” Wirbelsäule? Fremdmaterial (z.B. Klappenersatz, TEP, Demers)?
- L: ABx? Miktion (Menge)? Stuhl?
- E: Reisen?
- R: Impfungen? MRE-Risikofaktoren (Pflegeheim, Dialyse etc.)?
Workup
- Labor: BGA, 2-3 Paar BK (≥10 ml/Flasche), Profil “Sepsis”
- Bei Neutropenie oder Neugeborene: IL-6 nachfordern
- NLR
- Urin: U-Status immer +Kultur
- Weitere Materialgewinnung
- Sputum/TBS bei V.a. Pneumonie
- Abstriche: PCR COVID/Influenza, ggf. Multiplex respiratorische Erreger, tiefe Wundabstriche
- Katheter: +BK hieraus (Entnahmestelle angeben), ggf. Spitze ad MiBi
- LP: bei V.a. Meningitis (i.d.R. nach cCT)
- Aszitespunktion/Pleurapunktion
- VP-Shunt-Punktion (NCh)
- POCUS insb. zur DD andere Schockursachen
- Radiologie nach Verdacht, bei unklarem Fokus großzügig CT
- Fokussuche s.u.
Fokussuche (LUCCAASSS)
- Lung: Husten, Auswurf, Dyspnoe? LUS? CT Thorax?
- (Infarkt-)Pneumonie
- Pleuraempyem
- Urogenital: Dysurie? Flankenklopfschmerz? Sonografie Harnwege? U-Status + Kultur?
- HWI
- Prostatitis (nach DK-Fehllage)
- Fournier-Gangrän
- Epididymitis
- Cardiac: IVDU? Vorerkrankungen? Janeway, Osler, Splinter? Herzgeräusch? TTE (kein Ausschluss) / TEE?
- CNS: Meningismus? Lichtscheu? FND? cCT? LP? Shuntpunktion (NCh)?
- Meningitis / Enzephalitis
- Hirnabszess
- Spinaler epiduraler Abszess
- Shuntinfektion
- Abdomen: Untersuchung? Sonografie Abdomen? CT Abdomen? Aszitespunktion?
- Gallenerkrankungen
- Appendizitis
- Divertikulitis
- Perforation/Peritonitis
- SBP
- Toxisches Megacolon bei C. diff.
- Arthritis: Z.n. OP/Spritzen? POCUS MSK? Gelenkpunktion?
- Septische Arthritis
- Prothesen-Infekt
- Spine: Rückenschmerz? Z.n. OP/Spritzen? MRT?
- Spondylodiszitis
- Spinaler epiduraler Abszess
- Skin: Inspektion gesamtes Integument? ggf. gezielt CT
- Erysipel, Phlegmone, Gangrän
- Abszess
- Katheter-Infektion
- Wundinfektion
- Nekrotisierende Fasziitis
- Sonstiges:
- HNO
- Zähne
- Einliegende Fremdkörper (z.B. Spirale, Tampon, Shunt)
Kalkulierte ABx schwere Infektion
- Pneumonie → Pip/Taz 4.5 g i.v. + Azithromycin 500 mg p.o. (HAP: stattdessen + Ciprofloxacin)
- HWI → Pip/Taz 4.5 g i.v.
- Haut/Weichteile
- Nekrotisierende Fasziitis od. schwere/nekrot. Infektion: Meropenem 2 g + Clindamycin 600 mg i.v., Salzwasser +Doxycyclin, Süßwasser +Ciprofloxacin, RS ACh
- Erysipel, Phlegmone, schwerer Abszess: Ampicillin/Sulbactam 3 g i.v.
- Spritzenabszess IVDU: Clindamycin 600 mg q8h p.o. 5d
- Meningitis →
- ZNS-Abszess → RS NCh möglichst Punktion/OP vor ABx, ansonsten Ceftriaxon 2 g + Metronidazol 500 mg + Fosfomycin 5 g i.v.
- Sepsis ohne Fokus → Pip/Taz 4.5 g i.v.
- MRGN-Risiko: Meropenem 2 g i.v.
- V.a. MRSA: +Vancomycin, bei Fokus Lunge +Linezolid 600 mg i.v.
- Septischer Schock: Meropenem 2 g + Ciprofloxacin 400 mg i.v.
- Neutropenes Fieber wie Sepsis ohne Fokus, RS Häma/Onko
Anamnestisch Penicillin-Allergie? → Delabeling
- PEN-FAST 0 Pkt. → Allergie de-labeln, Beta-Laktam verabreichen
- PEN-FAST ≥1 Pkt. + anamnestisch schwere Anaphylaxie → Pencilline meiden + Cephalosporine möglichst auch
- PEN-FAST ≥1 Pkt. + anamnestisch leichte/mittlere Reaktion → Pencilline meiden + Cephalosporine Gen. 3/4/5 bei klarem Benefit / first choice trotzdem verabreichen1
Fokussanierung
- V.a. Katheter-Infektion ZVK/PiCC: BK hieraus, danach direkt entfernen, ggf. Spitze ad MiBi
- V.a. Port-Infektion: BK, Explantation ACh (bei schwachem Verdacht ggf. erst bei pos. BK)
- Abszess/Verhalt: Spülung/Drainage i.d.R. ACh, ggf. Endoskopie (z.B. Anastomoseninsuffizienz)
- Spondylodiszitis: OP UCh, bei FND/Querschnitt NCh
- Feuchte Gangrän: Debridement/Amputation GCh/ACh
- Infizierte Harnstauungsniere: Notfall-OP Uro
- Fournier-Gangrän: Notfall-OP Uro
- Nekrotisierende Fasziitis: Notfall-OP ACh
- Orbitaphlegmone: MKG
- Zahn-Abszess: MKG
- VP-Shunt-Infektion: NCh
- Prothesen-Infekt: Implantierende Fachrichtung
Stress-Dose Steroid
- Indikation:
- Chronische Cortison-Therapie / NNR-Insuffizienz
- Sepsis therapierefraktär auf NA ≥0.25 μg/kg/min >4h
- Schwere ambulant erworbene Pneumonie
- KI:
- Infektion mit Pilzen/Mycobakterien
- Immunsupp.
- Dosis:
- Hydrocortison 100 mg Bolus i.v.
- danach Perfusor 100 mg in 48 ml(!) mit LR 2 ml/h
Therapierefraktärer Schock Checkliste
- Ursache adressiert? Source Control für Sepsis, Thrombektomie für LAE etc.
- Metabolisch?
- Azidose: Isotones Bicarb, ggf. +Vasopressin
- NNR: Empirisch Hydrocortison 200 mg i.v.
- Hypocalcämie: Ca2+ Subst.
- Hypothyreose: ggf. auch empirisch T4 400 μg i.v.
- Hypothermie: Wärmen
- Anaphylaxie? a) von Beginn an, b) auf ABx → empirisch Adrenalin i.m./i.v.
- Toxine? inkl. reguläre Dosis Calciumantagonisten/Betablocker/Digitalis
- Blutung? z.B. GI-Blutung, retroperitoneal, SHT
- Obstruktiv?
- Klassiker/RUSH: Pneu, Perikarderguss, LAE
- PEEP reduzieren
- Abdominelles Kompartment: Blasendruck > 20 mmHg → Parazentese, Magensonde, Chirurgie
- Dynamic LVOTO: Vorlast↑, Nachlast↑, keine Inotropie, Tachy kontrollieren
- Kardiogener Schock: TTE → Intropie (a.e. Adrenalin)
- Zweite Diagnose? Premature Closure
- Fancy Therapien? ECMO, IABP, LAVD, etc.
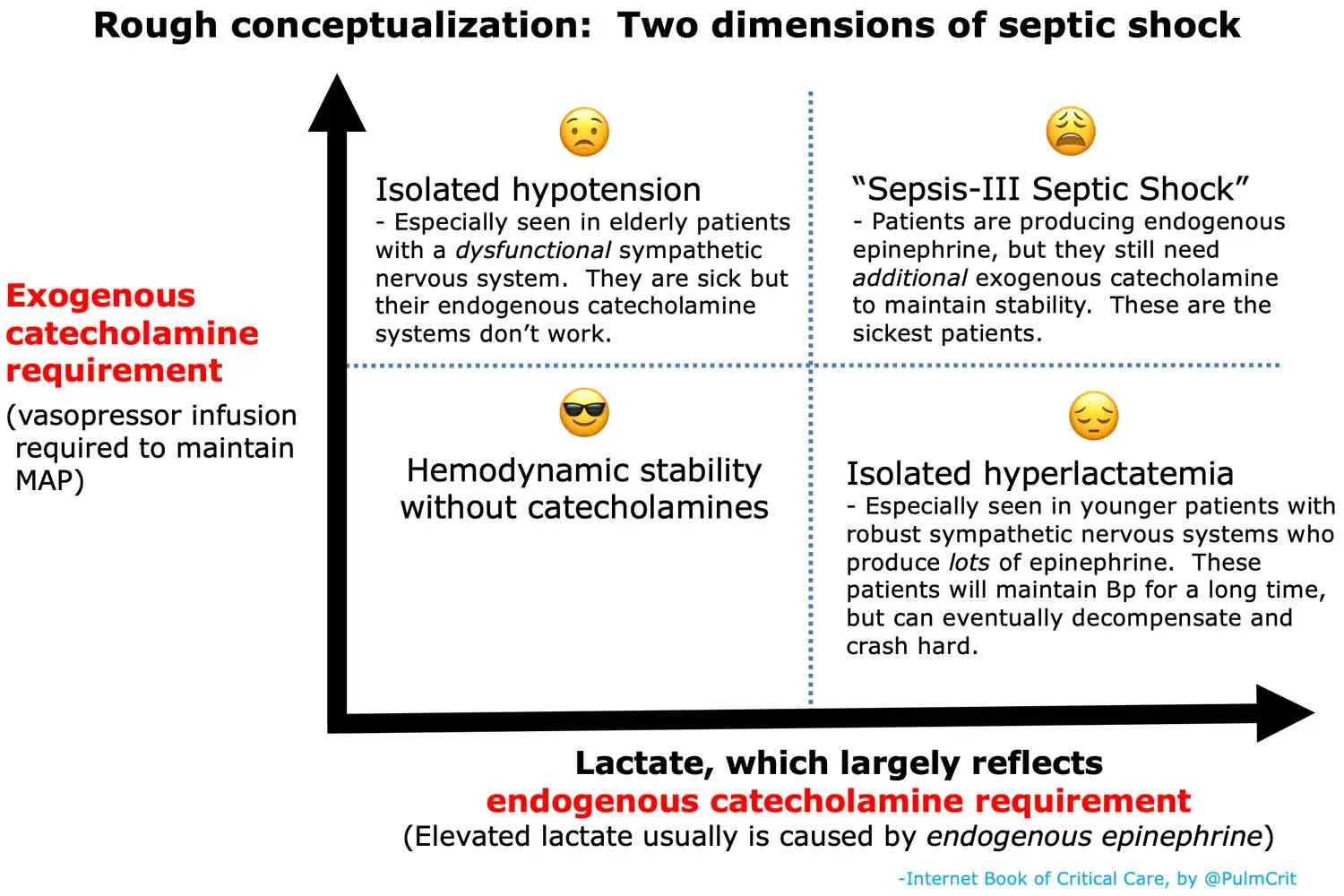
Septischer Schock Definition
Literatur
Patients with septic shock can have any of the following patterns hemodynamics (which we will explore in more detail): 1. Distributive shock with high cardiac output and low filling pressures (‘warm’) 2. Distributive shock with low cardiac output and low filling pressures (‘cold’ or sometimes referred to as ‘hypovolemic’ à not a volume issue but rather a low filling pressure) 3. Distributive shock with high cardiac output and HIGH filling pressures (‘high output failure’) 4. RV failure (high or low CO) 5. LV failure (high or low CO) 6. Biventricular failure (high or low CO) 7. Pericardial Effusions 8. Venous Congestion (this can be layered on to any of the phenotypes with higher filling pressures)
- PCT-Guided ABx Dauer ist sicher in Sepsis1
- Neue S3 LL2
- Früh Albumin kein Benefit3
- S3-Leitlinie Sepsis