Flowchart
flowchart TD Start(**Tachykardes VHF/VHFla**):::mStart --> ABCDE{{"**ABC-Instabil?**<br>Schock, Vigilanz↓, AP, Lungenödem"}}:::mCritical ABCDE -->|Ja| Bedarf{{**Bedarfstachykardie?**}}:::mImportant Bedarf -->|Nein| eKV(**elektr. Kardioversion**<br>in Analgosedierung) eKV --> SR{{**Sinusrhythmus?**}} SR --> |Nein| Korrektur("Patches optimieren (AP),<br>Elyte hochnormal,<br>1x MgSO4 2g i.v.",<br>ggf. Amiodaron 150 mg KI) Korrektur --> |max. 3x wiederholen<br>danach: RS Kardiologie| eKV Bedarf -->|Ja| U(**Ursache behandeln**<br>Bedarfstachykardie<br>akzeptieren) ABCDE --> |Nein| Bedarf2{{**Bedarfstachykardie?**}}:::mImportant Bedarf2 -->|Ja| U Bedarf2 -->|Nein|HF{{**HF ≥110/min**}} HF --> |Ja| FK(**Frequenzkontrolle**<br>Betablocker titriert p.o.) HF --> |Nein| Dispo(**Disposition**<br>ambulant möglich?) FK --> HF click ABCDE "/ABCDE" click eKV "/eKV"
Rapid Reference
- HF >>1501
- New-onset VHF
- Atrial Kick dependent Erkrankungen (Pulmonale Hypertonie, AS, MS, HFpEF)
- FBI (WPW+VHF)
- Frequenzkontrolle vs. Rhythmuskontrolle
- bei oligosympt. Älteren eher nur Frequenzkontrolle
- eKV bei stabilem VHF möglich?
- AK >3 Wochen (Adhärenz? Bei VKA: INR >2.0) oder
- Onset <12h oder Onset <48h + CHADS65 ≤2 (HFrEF, HTN, ≥65 J., Diabetes) oder
- TEE LAA-Thrombus negativ
- Elektrolyte?
- Volumenstatus?
- Sympathikotonus?
- Medikamente/Intox?
Workup
- Ätiologie:
- Herzinsuffizienz
- Ischämisch (KHK)
- Kardiomyopathie
- Elektrolyte (insb. HypoK+)
- RHB (LAE, COPD, Pulmonale Hypertonie)
- Myokarditis
- Valvuläres VHF: insb. Mitralklappenstenose
- Holiday-Heart-Syndrom: Paroxysmales VHF nach Alkoholexzess
- Labor: HypoK+? HypoMg2+? Hyperthyreose? ggf. Digitalis-Spiegel?
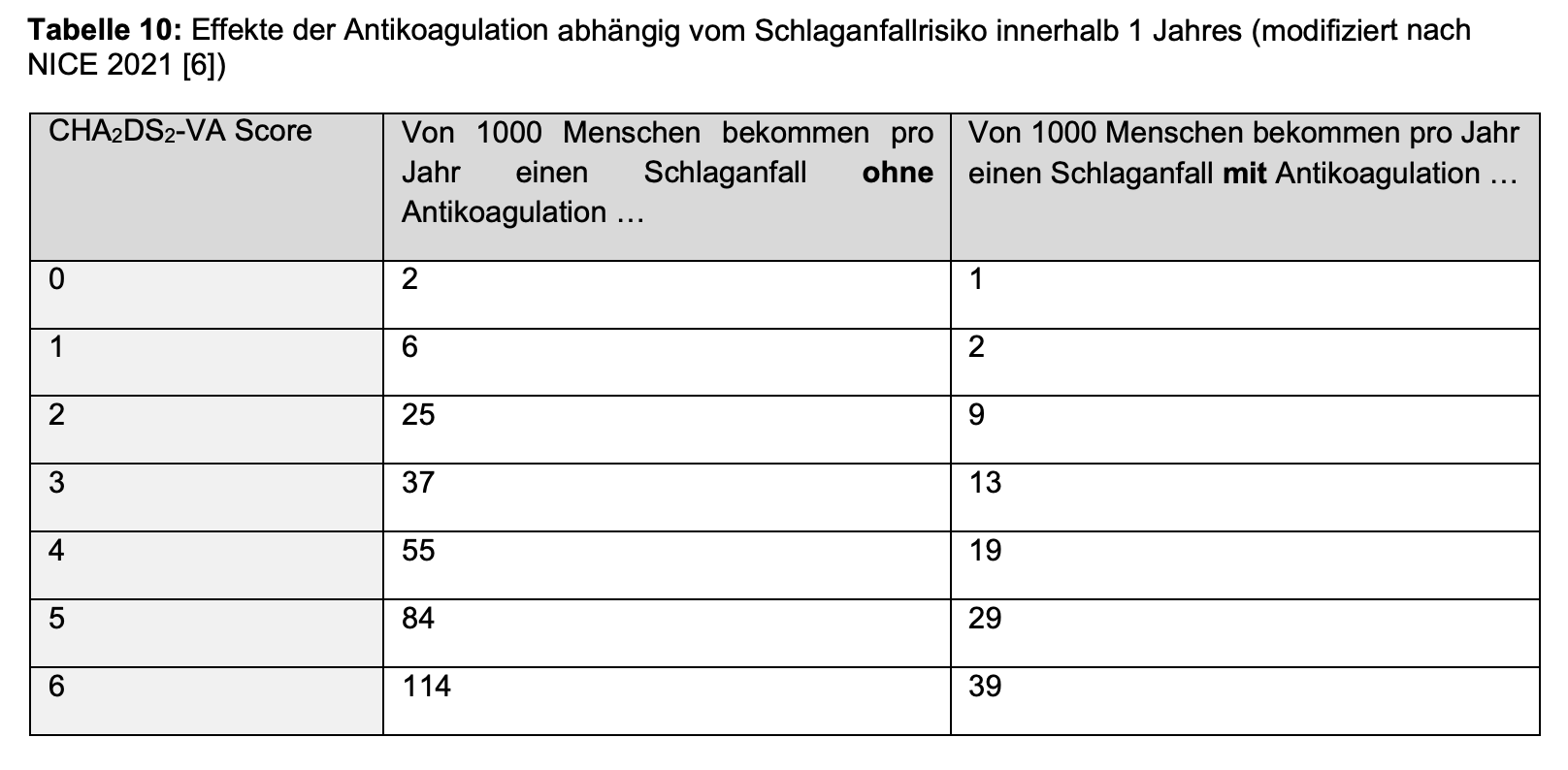
Antikoagulation bei VHF
Antikoagulation
Textbaustein Diagnose VHF
Aktuell: Intermittierendes/Persistierendes/Permanentes, bradykardes/normofrequentes/tachykardes Vorhofflimmern (VHF), ED ### - ##.##.####: CHA2DS2-VASc: ### - ##.##.####: eKV - ##.##.####: Ablation - OAK mit
Literatur
- S3-Leitlinie Vorhofflimmern
- Koffein verursacht wahrscheinlich zumindest kein VHF, in 1 RCT sogar geringere Recurrence2
Footnotes
-
HF 120-180 normalerweise maximal ohne AV-Block / neg. Dromotropie, bei >200/FBI DD VHF + WPW ↩
-
Wong CX. Caffeinated Coffee Consumption or Abstinence to Reduce Atrial Fibrillation: The DECAF Randomized Clinical Trial. JAMA. 2025 Nov 9:e2521056. doi: 10.1001/jama.2025.21056. Epub ahead of print. PMID: 41206802; PMCID: PMC12598581. ↩